Insulin is one of the most important medications nursing students must master, especially when it comes to onset, peak, and duration.
If you want a quick warm-up before diving in, try our NCLEX Insulin Mastery Quiz — it pairs perfectly with this guide.
Understanding how fast each insulin works, when it peaks, and how long it lasts can help you prevent hypoglycemia, match doses to meals, and keep patients safe.
These patterns may seem confusing at first, but once you learn them step by step, everything starts to make sense.
Some insulins act like sprinters… others prefer a slow, all-day walk.
What Is Insulin and Why Timing Matters
Insulin is a hormone that helps move glucose from the bloodstream into the cells, where the body can use it for energy.
Without enough insulin — or without insulin working correctly — blood glucose rises, leading to complications that affect the whole body.
Insulin Definition
Insulin acts like a “key” that unlocks cells so glucose can enter.
When insulin is given correctly, it keeps blood sugar steady and prevents dangerous highs and lows.
Why Insulin Onset, Peak & Duration Matter
Every insulin type works at a different speed.
The onset tells you when it starts working.
The peak tells you when it works the hardest.
The duration tells you how long it stays active.
Example:
A patient may become hypoglycemic if the insulin peak arrives earlier than expected — a common scenario when rapid-acting insulin is given without food ready.
If you want to build confidence in matching timing with technique, the Drug Administration Techniques Quiz is a helpful place to start.
What are the types of Insulin?
Insulin comes in five main categories, and each type works at a different speed.
Knowing whether an insulin acts fast, slow, or all day helps you predict timing, prevent hypoglycemia, and match doses to meals safely.
Insulin Categories Overview
| Type of Insulin | Action Speed | Common Examples |
|---|---|---|
| Rapid-acting | Very fast onset | Lispro, Aspart, Glulisine |
| Short-acting | Fast onset | Regular (Humulin R) |
| Intermediate-acting | Medium, steady action | NPH |
| Long-acting | Slow, all-day action | Glargine, Detemir |
| Ultra-long-acting | Very slow, very long | Degludec |
If you want extra practice identifying drug categories, the Drug Classification Quiz is a great study boost.
Insulin Onset, Peak & Duration
Understanding onset, peak, and duration is the key to giving insulin safely.
These three timing patterns tell you when insulin starts working, when it works the hardest, and how long it continues lowering blood glucose.
Even though insulin categories sound simple, the timing differences can change everything — from when a patient should eat, to when hypoglycemia can occur, to which type is safest for overnight control.
Below is your master comparison table.
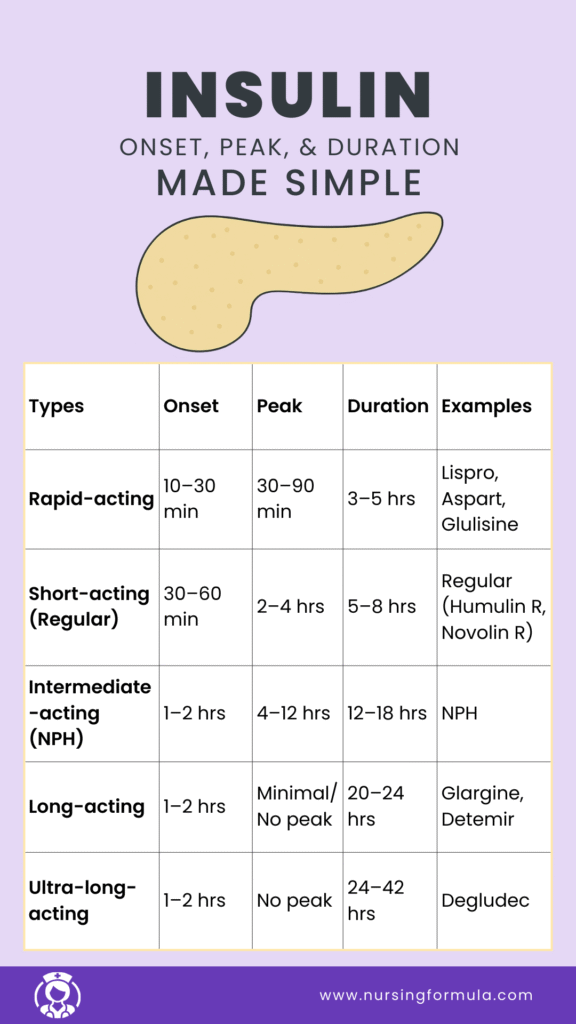
Five Types of Insulin Comparison Table
| Type of Insulin | Onset | Peak | Duration | Examples | Nursing Notes |
|---|---|---|---|---|---|
| Rapid-acting | 10–30 min | 30–90 min | 3–5 hrs | Lispro, Aspart, Glulisine | Give with food ready. Highest early hypoglycemia risk. Used for meals & correction doses. |
| Short-acting (Regular) | 30–60 min | 2–4 hrs | 5–8 hrs | Regular (Humulin R, Novolin R) | Can be given IV. Watch potassium. Good for DKA drips & pre-meal dosing. |
| Intermediate-acting (NPH) | 1–2 hrs | 4–12 hrs | 12–18 hrs | NPH | Cloudy. Roll gently. Higher mid-day hypoglycemia risk. Often used twice daily. |
| Long-acting | 1–2 hrs | Minimal/No peak | 20–24 hrs | Glargine, Detemir | Do NOT mix. Provides steady basal control. Best given at the same time daily. |
| Ultra-long-acting | 1–2 hrs | No peak | 24–42 hrs | Degludec | Very long coverage. Great for consistent baseline glucose. Lower hypoglycemia risk. |
Onset → When insulin starts working
This tells you how quickly you need to prepare the patient.
- Example: Rapid-acting insulin starts in minutes, so the patient must eat immediately.
- Example: Long-acting insulin has a slow onset, so food timing is not urgent.
Peak → When insulin is strongest
This is the MOST important time for hypoglycemia risk.
- Example: A patient who gets lispro and then delays their meal may crash during the 30–90 minute peak.
- Example: Glargine has no peak, so it keeps glucose steady overnight.
Duration → How long insulin keeps lowering glucose
This affects daily rhythms, overnight safety, and dose spacing.
- Example: NPH lasts long enough to cause mid-day hypoglycemia, especially if breakfast was small.
- Example: Degludec lasts up to 42 hours, making it helpful for patients with inconsistent schedules.
Here are a few short scenarios to help you understand this more clearly.
Example 1: Rapid-acting insulin
A patient receives lispro at 08:00. Breakfast is delayed.
By 08:40, the insulin is peaking, and the patient develops shakiness and sweating.
This is why food must be ready before giving rapid-acting insulin.
Example 2: Regular insulin (Short-acting)
You are running an insulin drip for a patient in DKA.
Regular insulin is used because its onset and action are predictable.
Example 3: NPH insulin
A patient who takes NPH at 07:00 becomes hypoglycemic at 12:00.
This matches its typical peak around 4–12 hours.
Example 4: Long-acting insulin
A patient takes glargine every night.
It has almost no peak, so it keeps blood sugar stable while they sleep.
Example 5: Ultra-long-acting insulin
A patient who sometimes forgets doses benefits from degludec’s 24–42 hour coverage.
It reduces the risk of overnight hypoglycemia and provides safety buffer.
1. Rapid-Acting Insulin
Rapid-acting insulin works very quickly. It is designed to control blood sugar right around mealtimes.
These insulins move into the bloodstream fast, peak early, and leave the body sooner than other types — which makes timing extremely important.
Common Rapid-Acting Insulins
These are the most commonly used rapid-acting insulins:
- Lispro
- Aspart
- Glulisine.
Rapid-Acting Insulin‘s Onset, Peak, and Duration
| Feature | Timing |
|---|---|
| Onset | 10–30 minutes |
| Peak | 30–90 minutes |
| Duration | 3–5 hours |
Remember:
Think of rapid-acting insulin as a sprinter — fast in, fast peak, fast out.
Rapid-Acting Insulin Example:
A patient receives lispro before breakfast. The food tray arrives late.
Because rapid insulin peaks so quickly, the patient may become hypoglycemic before eating.
This is why food must be ready before administering rapid-acting insulin.
Rapid-Acting Insulin Nursing Considerations
- Always check that meals are available before giving the dose.
- Watch closely for early hypoglycemia during the peak.
- Commonly used for mealtime coverage and correction doses.
- Teach patients to recognize signs of low blood sugar.
If you want extra practice monitoring medication effects, the Therapeutic Drug Monitoring Quiz is a great next step.
2. Short-Acting Insulin (Regular Insulin)
Short-acting insulin works a little slower than rapid-acting insulin, but it is very predictable.
This makes it useful for both mealtime coverage and certain IV treatments, especially in critical care settings.
Common Short-Acting Insulin
Regular insulin (Humulin R, Novolin R).
Short-Acting Insulin‘s Onset, Peak, and Duration
| Feature | Timing |
|---|---|
| Onset | 30–60 minutes |
| Peak | 2–4 hours |
| Duration | 5–8 hours |
Remember
Short-acting insulin is the fast jogger — predictable, steady, and reliable.
Short-Acting Insulin Example
Regular insulin is often used in IV drips for DKA because its onset and action are predictable. This makes blood glucose correction safer and easier to control.
Short-Acting Insulin Nursing Considerations
- Monitor potassium levels — insulin can shift potassium into cells.
- Check blood glucose frequently, especially during the peak.
- Can be administered IV when ordered.
- Ensure meal timing aligns with the insulin onset when given subcutaneously.
If you need more practice with potassium shifts and fluid balance, the Fluid and Electrolyte Balance Quiz is a helpful review.
3. Intermediate-Acting Insulin (NPH)
Intermediate-acting insulin provides longer coverage than rapid and short-acting insulins.
It is often used twice daily and plays a big role in maintaining daytime glucose control.
Why It’s Called NPH?
- Neutral → balanced pH
- Protamine → a protein added to slow absorption
- Hagedorn → named after Hans Christian Hagedorn, a scientist who helped develop it
The protamine makes the insulin cloudy and slows how fast it works — this is why you must roll the vial gently before drawing it up.
Common Intermediate-Acting Insulin
NPH insulin.
Intermediate-Acting Insulin’s Onset, Peak, and Duration
| Feature | Timing |
|---|---|
| Onset | 1–2 hours |
| Peak | 4–12 hours |
| Duration | 12–18 hours |
NPH Memory Trick
NPH = “Not fast, not long — right in the middle.”
Remember
NPH is the “steady middle” insulin — not fast, not slow, but right in the middle with a long, wide peak window.
Example
A patient takes NPH at 07:00 and becomes hypoglycemic around noon. This matches the typical peak time, which is when NPH is strongest.
Intermediate-Acting Insulin Nursing Considerations
- Roll the vial gently before drawing up the dose.
- Monitor for hypoglycemia during the peak hours.
- Often given twice daily as part of a mixed insulin regimen.
- Teach patients how peaks affect meal timing and snacks.
If you want to sharpen your skills with overlapping medications and timing, the Medication Reconciliation Quiz is a great fit.
Quick NPH Comparison
| Feature | NPH (Intermediate-Acting Insulin) |
|---|---|
| Appearance | Cloudy → must roll the vial |
| Onset | 1–2 hours |
| Peak | 4–12 hours (big hypoglycemia window) |
| Duration | 12–18 hours |
| Given | Usually twice daily |
| Mixing | Can mix with Regular insulin (clear to cloudy) |
| Key Concern | Midday hypoglycemia |
4. Long-Acting Insulin
Long-acting insulin provides steady, round-the-clock glucose control.
It works slowly, with little to no peak, making it dependable for basal (background) coverage throughout the day and night.
Common Long-Acting Insulins
Glargine and Detemir.
Long-Acting Insulin‘s Onset, Peak, and Duration
| Feature | Timing |
|---|---|
| Onset | 1–2 hours |
| Peak | Minimal or none |
| Duration | 20–24 hours |
Remember
Long-acting insulin acts like an all-day bodyguard — stable, smooth, and always on duty.
Long-Acting Insulin Example
Glargine is often used for baseline glucose control, even when patients are not eating.
Its steady action helps prevent overnight highs and keeps fasting glucose stable.
Long-Acting Insulin Nursing Considerations
- Do NOT mix long-acting insulin with any other insulin in the same syringe.
- Give at the same time each day for consistent coverage.
- Monitor fasting glucose to adjust dosing.
- Low peak means lower hypoglycemia risk — but still monitor closely.
For extra practice with insulin safety and high-risk medications, the High-Risk Drug Safety Quiz is a helpful review.
5. Ultra-Long-Acting Insulin
Ultra-long-acting insulin provides the longest and most stable basal coverage.
It keeps blood glucose steady for more than 24 hours, making it one of the easiest insulins for patients to manage.
Common Ultra-Long-Acting Insulin
Degludec.
Ultra-long-acting insulin’s Onset, Peak, and Duration
| Feature | Timing |
|---|---|
| Onset | 1–2 hours |
| Peak | No significant peak |
| Duration | 24–42 hours |
Remember
Ultra-long-acting insulin is the marathon runner — slow, steady, and built to last.
Ultra-long-acting insulin Example
Degludec is helpful for patients who sometimes forget doses.
Its long, steady control provides a safety buffer and reduces the risk of glucose swings.
Ultra-long-acting insulin Nursing Considerations
- Given once daily in most cases.
- Provides smooth basal coverage without peaks.
- Lower risk of nighttime hypoglycemia.
- Supports flexible dosing schedules when needed.
For more practice understanding long-duration medications and steady infusions, the Infusion Pump Programming Quiz is a useful review.
Sample Nursing Scenarios
Here are a few short scenarios to help you see how insulin timing affects real bedside care.
These simple examples make onset, peak, and duration easier to apply in practice.
Scenario 1 — Rapid-Acting Insulin (Lispro)
A patient receives lispro at 08:00 for breakfast coverage.
The meal tray is delayed.
By 08:40, the insulin is already peaking, and the patient becomes shaky and pale.
The nurse immediately checks glucose and provides fast-acting carbohydrates.
Teaching point: Rapid insulin requires food ready before administration because the peak comes fast.
Scenario 2 — Short-Acting Insulin (Regular Insulin)
A patient in DKA is placed on a continuous insulin drip.
Regular insulin is used because it has a predictable onset and steady action.
Potassium levels drop as insulin therapy begins.
The nurse prepares to replace potassium based on lab orders.
Teaching point: Regular insulin is used in IV drips and requires frequent potassium monitoring.
Scenario 3 — Intermediate-Acting Insulin (NPH)
A patient takes NPH at 07:00 each morning.
At 12:00, they report dizziness, sweating, and irritability.
Their blood glucose is 58 mg/dL.
This matches the typical 4–12 hour peak of NPH.
Teaching point: NPH peaks at midday → highest hypoglycemia risk in late morning to early afternoon.
Scenario 4 — Long-Acting Insulin (Glargine)
A patient takes glargine every night at 21:00.
They are admitted with new-onset nausea and poor appetite.
The nurse still gives glargine because it provides basal coverage and does not depend on meals.
Blood glucose stays steady overnight with no major drops.
Teaching point: Long-acting insulin has minimal peak and maintains baseline glucose, even when patients aren’t eating.
Scenario 5 — Ultra-Long-Acting Insulin (Degludec)
A patient frequently forgets their insulin doses at home.
The provider switches them to degludec because it lasts 24–42 hours and offers more flexibility.
When the patient takes a dose later than usual, their glucose still remains stable.
Teaching point: Ultra-long-acting insulin provides very consistent coverage with lower hypoglycemia risk and flexible timing.
Scenario 6: Patient Going NPO
A patient is scheduled for surgery and is now NPO.
They normally take rapid-acting insulin with breakfast.
Because they cannot eat, giving their usual dose would raise the risk of hypoglycemia during the peak.
In this case, the nurse holds the rapid insulin and checks the provider’s instructions for adjusted dosing.
Scenario 7: Hypoglycemia After Peak
A patient took NPH at 07:00.
At 12:00, they report feeling shaky and sweaty.
This lines up with the NPH peak, which often happens midday.
The nurse checks blood glucose and treats hypoglycemia promptly.
Scenario 8: New Diabetic Learning Meal Timing
A newly diagnosed patient receives lispro with lunch.
They begin eating slowly and plan to save half the meal for later.
Because lispro peaks quickly, the nurse teaches the patient to eat enough carbohydrates immediately to match the insulin’s action.
If you want to practice similar scenarios in a quiz format, the NCLEX-Style Drug Quiz is a great place to start.
Safety: Hypoglycemia & When to Hold Insulin
Insulin safety starts with knowing when to give it and when to pause.
Hypoglycemia can happen quickly, especially during peak times, so nurses must check blood glucose, assess symptoms, and think ahead.
Hypoglycemia Signs to Watch For
- Shakiness
- Sweating
- Irritability
- Hunger
- Headache
- Confusion
- Weakness
Even long-acting insulins can cause low blood sugar, especially if meals are skipped, patients are NPO, or doses overlap.
When to Hold Insulin
You should hold insulin and reassess when:
- Blood glucose is below 70 mg/dL
- The patient is NPO and takes mealtime insulin
- The patient shows clear hypoglycemia symptoms
- A rapid-acting dose is ordered but no food is available
- The provider has adjusted or changed the dose
- The patient refuses to eat after the insulin has already been drawn up
Example
A patient has a blood glucose of 65 mg/dL before their breakfast insulin.
The nurse holds the dose, treats the hypoglycemia, and rechecks blood glucose before giving any insulin.
Key Insulin Safety Reminders
- Always know the peak time before giving the insulin.
- “Check twice” for high-risk doses or patients with unpredictable eating patterns.
- Reassess blood sugar after treating hypoglycemia.
- Review the insulin order if the patient’s condition changes unexpectedly.
If you want to practice emergency situations like this, the Free Emergency Drug Quiz is a useful review.
Insulin Mnemonics: Easy Memory Tricks for Onset, Peak & Duration
Insulin timing becomes much easier when you use simple memory cues.
These short mnemonics help you remember onset, peak, and duration without feeling overwhelmed.
Rapid-Acting Insulin
“15 minutes feels like 15 seconds.”
Rapid-acting insulin works almost immediately, so food must be ready.
Short-Acting Insulin (Regular)
“Regular insulin runs regular schedules.”
Predictable onset, predictable peak, predictable duration.
Intermediate-Acting Insulin (NPH)
“NPH = Noon Peak Happens.”
NPH often peaks around lunchtime → highest hypoglycemia risk.
Long-Acting Insulin
“Long-acting = Long and Level.”
Minimal peak. Smooth, steady coverage.
Ultra-Long-Acting Insulin
“Degludec = The Ultra Marathon.”
Lasts 24+ hours with no strong peak.
Universal Peak Reminder
“Peak = Panic potential.”
Always check blood glucose during insulin peak times.
Insulin Mnemonics Table
| Insulin Type | Mnemonic | Meaning / Memory Aid |
|---|---|---|
| Rapid-acting | “15 minutes feels like 15 seconds.” | Works fast → food must be ready. |
| Short-acting (Regular) | “Runs regular schedules.” | Predictable onset and peak → easy to time with meals. |
| Intermediate (NPH) | “Noon Peak Happens.” | Usually peaks midday → risk for hypoglycemia. |
| Long-acting | “Long and Level.” | Smooth, steady coverage with little to no peak. |
| Ultra-long-acting | “Ultra Marathon.” | Very long duration → stable basal control. |
| Peak reminder (all types) | “Peak = Panic potential.” | Highest risk of low blood sugar at the peak. |
If you want to build even stronger memory shortcuts, the Drug Mnemonics Quiz is a fun way to practice.
Related Drug-Class Guides to Strengthen Your Pharmacology Understanding
If you want to build a stronger foundation in medication timing, safety, and mechanisms, these drug-class guides pair well with what you learned about insulin.
Each one breaks down complex concepts into simple patterns you can remember and use in real clinical practice.
- Beta Blockers Made Simple: MOA, Side Effects & Nursing Implications
- ACE Inhibitors vs ARBs: What’s the Difference?
These articles help you compare insulin with other high-yield medication groups and build a deeper understanding of how drug classes fit together in nursing care.
What You’ve Learned
Here’s a simple recap to help you remember the key points on insulin onset, peak, and duration:
- Insulin works at different speeds depending on the type.
- Onset tells you when insulin starts lowering glucose.
- Peak is the highest hypoglycemia risk — always watch closely.
- Duration tells you how long the insulin stays active.
- Rapid-acting insulin works fast and needs food ready.
- Short-acting insulin is predictable and used in DKA drips.
- NPH has a midday peak, which increases hypoglycemia risk.
- Long-acting insulin gives steady, all-day coverage with minimal peak.
- Ultra-long-acting insulin provides smooth, flexible basal control.
- Knowing timing patterns helps you give insulin safely and prevent low blood sugar.
- Memory tricks make insulin easier to understand and recall during exams.
- Real-world scenarios help connect timing with bedside decision-making.
If you want extra practice with core medication math skills, the Dosage Calculation Quiz is a great place to start.
To build confidence in pediatric insulin dosing, you can try the Pediatric Dosage Calculation Quiz.
For a quick review of IV timing and rate control, the Free IV Drip Rate Quiz is helpful.
And for broader pharmacology reinforcement, the Anticoagulant & Antiplatelet Drug Quiz is a solid next step.


